Our technology
medLYTIC Labs aim to revolutionize medical decision-making during DIAGNOSIS & INVASIVE treatment of coronary artery disease (CAD) with the application of ultra-fast numerical computer models
Cardiovascular disease (including heart disease and other arterial occlusive diseases) is the world’s No1. Killer accounting for nearly one third of global deaths worldwide. Atherosclerosis produces stenoses in the coronary arteries that impede blood flow and oxygen delivery to the myocardium, resulting in ischemic coronary artery disease.
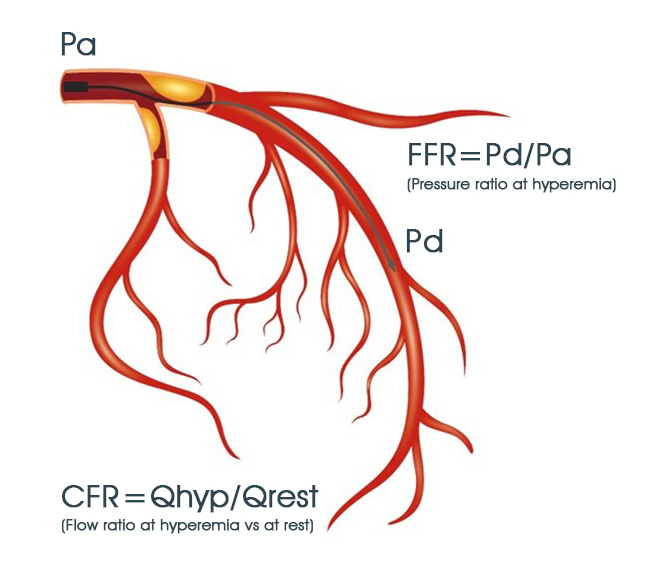
Coronary angiography allows for evaluation of the anatomical characteristics of arterial stenoses but is often inaccurate in identifying truly functionally significant coronary artery stenoses. Fractional Flow Reserve (FFR) is a hemodynamic index that quantifies the functional severity of a coronary artery stenosis and is defined as the ratio of distal pressure Pd versus proximal mean arterial pressure Pa at hyperemia.
FFR assesses the severity of an epicardial stenosis, whereas coronary flow reserve CFR defined as the ratio of coronary blood flow at hyperemia versus at rest helps assess the combined severity of proximal epicardial and distal microvascular disease.
Current guidelines recommend the use of FFR in identifying functionally significant epicardial coronary artery stenoses and determining the need for percutaneous coronary interventions (PCI) with balloons and stents. Established methods for FFR measurement mandate the invasive use of a guidewire along with the administration of pharmacological vasodilators that produce patient discomfort.

Invasive wire FFR has been shown to reduce future deaths by approximately 25%, recurrent myocardial infarctions by approximately 25% and heart related adverse events by 15%. However, because FFR measurements are invasive with some inherent risk and discomfort, healthcare professionals apply the method in less than 15-20% of the eligible cases.
On the contrary, Image-based computer methods have emerged for computer simulation of FFR, but they routinely rely on a three-dimensional reconstruction of the coronary arterial tree, they cannot reliably simulate hyperemia and they are uniformly time-consuming in the order of several minutes or even hours per image-reconstruction and FFR calculation. All the latter are major drawbacks restricting the clinical applicability and patient throughput in modern catheterization laboratories.